- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

This gentleman has a significant lumbar herniated disc with a positive well straight leg raise test. In this evaluation I test his deep tendon reflexes, sensation, muscle strength, and perform a straight leg raise test, Braggards's test and Well straight leg raise test.
✅ Support OEP: https://paypal.me/OrthoEvalPal?locale.x=en_US
✅ OEP Website: https://orthoevalpal.com/
✅ Online Coaching: https://orthoevalpal.com/coaching
✅ OEP Podcasts: https://orthoevalpal.com/podcast
▶▶ Like us on facebook: https://www.facebook.com/OrthoEvalPal
▶▶ Follow on Instagram: https://www.instagram.com/
▶▶ Follow on Twitter: https://twitter.com/home
✔ Get our NEW downloadable 1.5 hour shoulder anatomy with cadaver dissection lecture: http://www.meorthopedicseminar....s.com/shop/shoulder-
✔Get our NEW downloadable 7.5 hour cervical and lumbar continuing ed course: http://www.meorthopedicseminar....s.com/shop/rehabilit
✔Get our NEW downloadable 6.0 hour shoulder continuing ed course: http://www.meorthopedicseminar....s.com/shop/comprehen
Interested in our Sponsor Product
EZ Slant (http://ezslant.com/)
Check out our new OEP merchandise: 👚👕☕️https://www.youtube.com/channe....l/UC76MsdkAQaBkCb35K
#wellstraightlegraise #herniateddisc #LBP #lowbackpain #OrthoEvalPal #SpecialTests #Orthopedics #physicaltherapy #physicaltherapytests #athletictraining

Be sure to have your teenager checked for hernias as they may be malevolent, Dr. Honaker gives us some insight as to why this is an important thing to have done.

Patient Glenn Williams had a hernia measuring 20cm x 30cm. Consultant Graham Offer has performed ground breaking surgery to help Glenn.

Dr. Ankur Gupta of the Virginia Eye Institute discusses LASIK eye surgery as a method of correcting refractive errors. LASIK was first performed in Virginia on an FDA-approved laser by a VEI surgeon in 1996. Today, Virginia Eye Institute offers both conventional LASIK and custom LASIK with the bladeless IntraLase laser to precisely sculpt your cornea to correct refractive errors.
For more information on the services and procedures offered at Virginia Eye Institute please visit: https://goo.gl/6nX4RZ
THE CONTENT IN THIS VIDEO IS GENERAL IN NATURE AND DOES NOT SUBSTITUTE PROFESSIONAL MEDICAL ADVICE. The content on our website including, but not limited to, text, images, and videos is for informational and educational purposes only. Although we work hard to provide accurate general information, it is not a substitute for professional medical advice or consultations with healthcare professionals, and does not establish any kind of provider-patient relationship. Our website information is not intended to make any promises about the results of our products and services. We are not liable for actions taken based on content found on our website. If you are seeking medical advice, diagnoses, or treatment, we encourage you to call 804-287-2020 to make an appointment with one of our providers for your individualized care plan.

His father, Dr. Joseph Dello Russo, helped turn Lasik eye surgery into the widespread procedure it is today. Now he explains a new technique and how it differs.


LASIK is one of the most popular elective surgeries in the United States with 95% of patients walking away satisfied with their vision, according to one FDA study. But like with any surgery, there are risks.

On this week's episode of Macro Beauty, we follow a young woman on her journey to getting Lasik eye surgery. She opts for this corrective vision procedure and we captured it up close. Watch this video to see what the process is really like!
https://maloneyvision.com/
ABOUT SERIES
We're getting up close and personal into all things beauty. Have you ever wondered whether or not waterproof mascara really works? Or been intrigued with tattooing your eyebrows? We'll show you this process like you have never seen it before!
ABOUT REFINERY29
Refinery29 is a modern woman's destination for how to live a stylish, well-rounded life. http://refinery29.com/
RELATED CONTENT
Why I Got This 15 Minute Nose Job
https://youtube.com/watch?v=_TGq8Uuvf0w
Microblading Permanent Eyebrow Tattoo Up Close
https://youtube.com/watch?v=HhdTcySV9zo
How To Get A Nose Piercing With Brian Keith Thompson Of Body Electric
https://youtube.com/watch?v=OPhvc_4kjas
SEE MORE REFINERY29 VIDEOS
http://refinery29.com/video
SUBSCRIBE TO REFINERY29
Subscribe to the Refinery29 channel: http://bit.ly/subscribe-to-r29
For the latest trends and videos, visit: http://refinery29.com
Like Refinery29 on Facebook: https://facebook.com/refinery29
Follow Refinery29 on Twitter: https://twitter.com/refinery29
Heart Refinery29 on Instagram: https://instagram.com/refinery29/
TALENT
Follow The Maloney Shamie Vision Institute on Instagram: https://instagram.com/maloneyvision/
Follow Emily on Instagram: https://instagram.com/emmy_free/
Follow Unbothered on Instagram: https://instagram.com/r29unbothered/
Follow OnHerTurf on Instagram: https://instagram.com/onherturf/
Follow Refinery29 on Instagram: https://instagram.com/refinery29/

If you are tired of dealing with glasses or squinting to read signs in the distance, then you should consider LASIK Eye Surgery. In this outpatient refractive procedure, lasers are used to correct vision issues by changing the structure of the cornea. This may entirely eliminate reliance upon glasses or contacts. In this interactive LASIK Eye Surgery, you will assist in numbing the patient’s eye and cleaning the area for the procedure. With a speculum, you will hold the eye open, mark the cornea using a water-soluble ink, then attach a suction ring to it. After that, a specialized blade device is used to cut into the corneal flap and peel it back so that the laser can clear away corneal tissue underneath. This process corrects the shape of the cornea in less than a minute before putting the corneal flap back in place. After the procedure, we will go over LASIK Eye Surgery recovery instructions. Scrub in and let’s get started!

Note: This video contains graphic surgical footage so viewer discretion is advised.
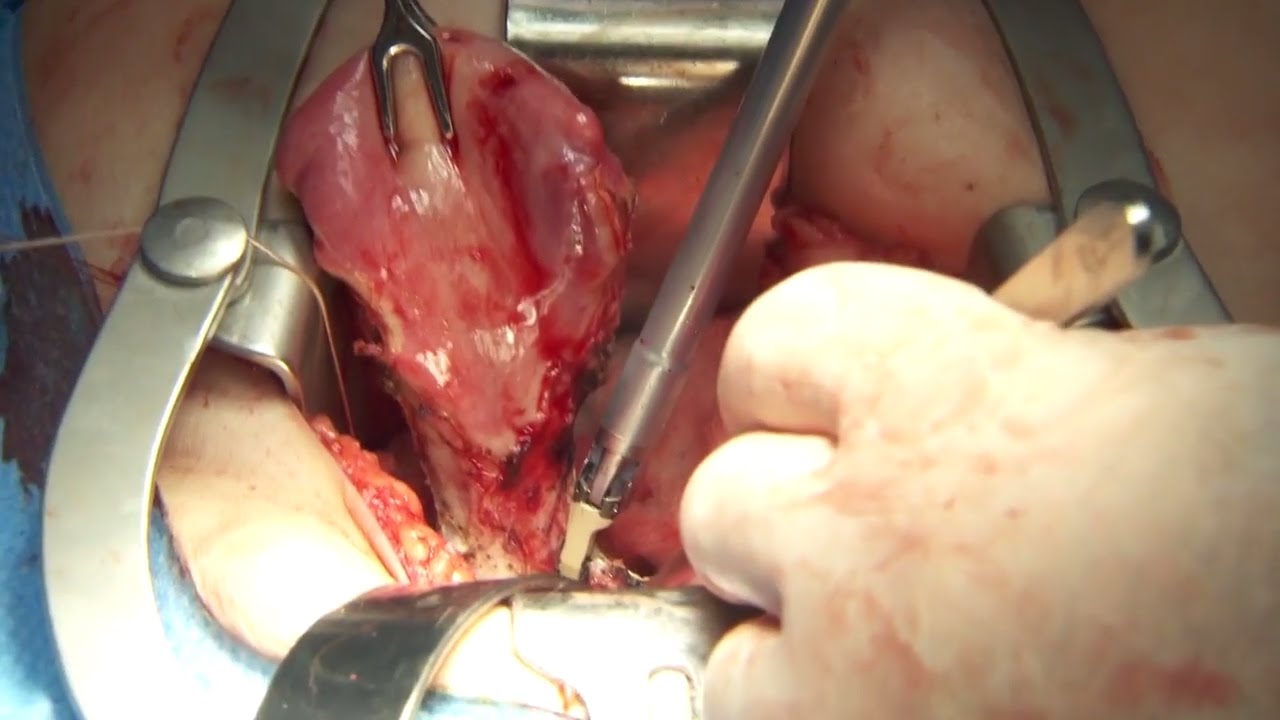
Director of the Penn Orthopaedics Robotics and Navigation Program, Dr. Christopher Travers, discusses robotic joint replacement surgery, which is one of the multiple options that Penn Orthopaedics offers for joint replacement surgery. He walks through a robotic knee replacement surgery, discussing what the procedure is, how it differs from traditional joint replacement surgery, and the benefits.
Refer a patient (physicians only):
https://www.pennmedicine.org/refer-your-patient
Learn more about the Penn Joint Replacement Program:
https://www.pennmedicine.org/f....or-patients-and-visi
Learn more about Dr. Travers:
https://www.pennmedicine.org/providers/profile/christopher-travers?fadf=pennmedicine&keyword=travers
#RoboticSurgery #JointReplacementSurgery #KneeReplacement #SurgicalFootage
Timothy Lovell, MD, an orthopedic surgeon, talks to Spokane, WA knee replacement surgery patients about the procedure, possible risks and complications of surgery, and about your recovery time.
Dr. Lovell addresses anesthesia, the size and location of the incision, and shows you what the knee replacement ball and socket joint looks like. He'll talk about the recovery process; using a crutches, a walker or a cane to get around; movements to avoid; and how long it takes to feel better and return to your normal, active life.
To learn more about Dr. Lovell, visit http://washington.providence.o....rg/find-a-provider/l
And, to learn more about having orthopedic surgery in Spokane, WA, visit http://washington.providence.o....rg/clinics/providenc

Knee replacement involves replacing a knee joint that has been damaged or worn away, usually by arthritis or injury. Find out more here: http://bit.ly/MAdfmE
The content is intended for general information only and does not replace the need for personal advice from a qualified health professional.

Care for Your Knee After Knee Replacement Surgery
In this video, Dr. Mark Hammerberg, provides details on two important activities to help during recovery from knee replacement surgery.
Denver Health's Orthopedics department offers many different types of treatments to help you, including surgical and non-surgical options. To find out if surgery is right for you, visit DenverHealth.org/Orthopedics or call 303-602-1590 to make an appointment.

Outpatient -- or same-day -- knee replacement surgery is more convenient than traditional knee replacement surgery and often can help you recover faster.
Outpatient -- or same-day -- knee replacement surgery is more convenient than traditional knee replacement surgery and often can help you recover faster. At Duke Ambulatory Surgery Center Arringdon, your knee replacement will be followed immediately by physical therapy to get you moving and start your recovery process right away. Our expert joint replacement team ensures your knee replacement surgery is safe and effective so you can return to the comfort of your home as soon as possible.


Warren Pettaway of Detroit knew he needed to have his left knee checked out when he could no longer keep up while officiating basketball. The pain got so bad that running up and down the court or quickly changing directions was too much for him to continue doing what he loved.Only three weeks post-surgery, Warren is ready to get back in the game. He is able to move without issue and is getting things done around the house. He makes sure to do his therapy as directed and is exercising on his own in the gym. To learn more visit https://www.henryford.com/serv....ices/joint-replaceme

Dr. James Wall performs a bilateral inguinial hernia repair surgical procedure.
Featured:
James Wall, MD
Assistant Professor of Surgery, Pediatric Surgery
Assistant Professor of Bioengineering (By Courtesy)
Lucile Salter Packard Children's Hospital
Micaela Esquivel, MD
Chief Resident of General Surgery

Carpal tunnel release (part 1). Skin incision and retraction. Procedure performed by Deepak Kapila, MD, Broward Health, Fort Lauderdale, FL. Courtesy of BroadcastMed (http://ortho.broadcastmed.com/....4229/videos/carpal-t
There are hundreds more procedural videos as well as news, features, resources and references on Medscape.com. Join today for free.

Shane Shapiro, M.D., orthopedic physician at Mayo Clinic in Florida, performs a bone marrow aspiration and concentration for BMAC/stem cell injection into arthritic knees. This procedure is part of a Mayo Clinic IRB approved, FDA monitored clinical research trial which can be searched on at http://ClinicalTrials.gov.
Mayo Clinic and the Mayo Center for Regenerative Biotherapeutics is studying biologically based non-surgical treatments for osteoarthritis. One such treatment is the harvesting of the patient's own stem cells from their bone marrow.
"In our procedure we draw cellular rich bone marrow from both sides of the pelvis. We then filter the resulting product and concentrate the stem cells and their corresponding growth factors. Using an ultrasound to image the knee joint, we are then able to precisely inject the cells into the arthritic knee. We are currently demonstrating that this procedure is safe and can relieve pain. We also hope to be able to slow the progression of the degenerative joint disease and perhaps one day regrow cartilage in the arthritic joint."
------
Hear Dr. Shapiro discus this procedure in detail here: http://youtu.be/8Djpsc66hKI
Learn more about the Mayo Clinic Center for Regenerative Biotherapeutics here: http://goo.gl/rnRdtU
------
Mayo Clinic...
On Facebook: http://Facebook.com/MayoClinic
On Twitter: http://twitter.com/MayoClinic
On Google+: http://google.com/+MayoClinic
On Instagram: http://instagram.com/MayoClinic
On Pinterest: http://Pinterest.com/MayoClinic
On YouTube: http://YouTube.com/MayoClinic
On the blogs: http://connect.MayoClinic.org
Olympus has extended the value of its award-winning combined surgical energy device, THUNDERBEAT, to open surgical procedures. Watch Dr. Francois Blaudeau master use of THUNDERBEAT Open Extended Jaw (OEJ) in a total abdominal hysterectomy.
http://medical.olympusamerica.com/products/thunderbeat?utm_source=youtube&utm_campaign=Total%20Abdominal%20Hysterectomy%20Surgery%20-%20THUNDERBEAT&utm_medium=description&utm_term=energy&utm_content=surgical
