- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

childbirth twin baby

Alexandra J. Golby, MD, Director, Image-guided Neurosurgery at Brigham and Women’s Hospital, discusses technological advancements to improve the precision of surgery to remove brain tumors.
It’s estimated that each year nearly 80,000 people are diagnosed with primary brain tumors and 100,000 with metastatic brain tumors. Nearly everybody is at risk for developing a brain tumor. Brain tumors can affect people from childhood to the last years of their lives. Men are slightly more affected than women and the causes of most brain tumors are not known.
There are a number of unique challenges in treating brain tumors. One challenge is that primary tumors can have indistinct margins that are difficult to see. Another challenge is that the tissue around a brain tumor is uniquely important and may impact things like language, visual and motor function.
The AMIGO Suite, opened in 2011 at Brigham and Women’s Hospital, is the Advanced Multimodality Image Guided Operating Suite. It's an NIH-funded national center which was developed with the goal of translating technological advances into improvements in surgical and interventional care for patients. In the AMIGO Suite, there is an intraoperative MRI scanner which can be brought in and out of the operating room during surgery to help surgeons visualize a patient’s tumor better.
Image-guided surgery uses the information obtained from advanced imaging and translates that into the planning and execution of surgery by acquiring high resolution and specialty structural images of the brain and also functional images of the brain. These images can be registered to one another and then to the patient's head during surgery. This allows surgeons to pinpoint the location of the tumor as well as the areas that we would like to preserve, areas that serve critical brain functions are located.
One of the big challenges, even with image-guided surgery, is that as we perform the surgery, the configuration of the brain is changing, and we call that brain shift. And it's due to changes in the brain itself and also as we remove tissue, things are constantly shifting and moving. When we're talking about doing brain tumor surgery, a few millimeters of movement can be a big difference. How to measure and track brain shift is an important area of research and a number of technologies are being studied to understand how to measure brain shift during surgery.
The development of various intraoperative imaging technologies allows surgeons to provide the most accurate surgical treatment for each individual patient.
Learn more about precision brain surgery at Brigham and Women’s Hospital:
https://www.brighamandwomens.o....rg/neurosurgery/brai

Watch that Baby Abortion Medical Procedure

Gynecological Examination

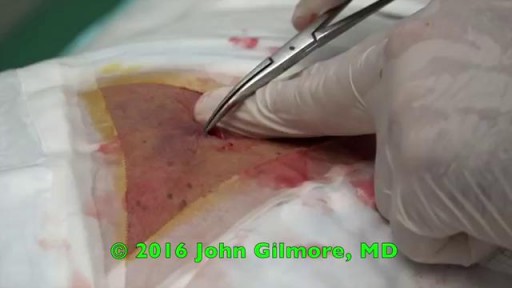
This patient presented to the ER for umbilical pain and had a history of umbilical hernia. He was concerned about the possibility of incarceration of the hernia.
In this video we explain how the clinical exam helps to differentiate a simple painful hernia from an incarcerated one.
***Thanks to the patient for sharing his history and exam with YouTube world***

The products of a surgical abortion.

The umbilical cord is wrapped around the baby's neck in about 25% of deliveries. If loose, it usually has no impact on the delivery. If tight, it may need to be relieved before delivery of the baby can proceed safely

A great video showing the multiple presentations of the baby which the doctor may encounter while delivery like breech presentation..etc

Ganglion Cyst Volar Wrist Removal Ganglion cysts are noncancerous lumps that most commonly develop along the tendons or joints of your wrists or hands. They also may occur in the ankles and feet. Ganglion cysts are typically round or oval and are filled with a jellylike fluid. Small ganglion cysts can be pea-sized, while larger ones can be around an inch (2.5 centimeters) in diameter. Ganglion cysts can be painful if they press on a nearby nerve. Their location can sometimes interfere with joint movement. If your ganglion cyst is causing you problems, your doctor may suggest trying to drain the cyst with a needle. Removing the cyst surgically also is an option. But if you have no symptoms, no treatment is necessary. In many cases, the cysts go away on their own.
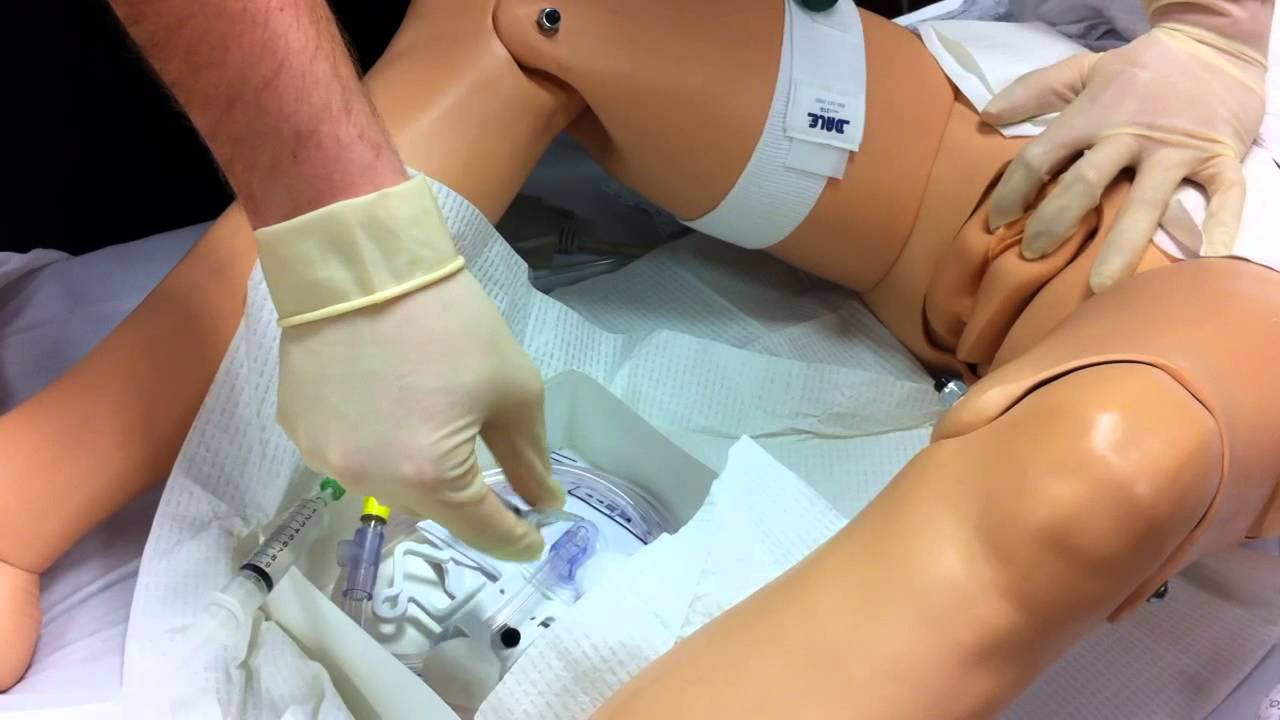
Watch that Female Foley Genital Catheter Insertion Procedure

A VCUG (Voiding Cystourethrogram) is a test that looks at how well your child's kidneys, ureters and bladder are working. Your child's kidneys make urine. The urine flows from the kidneys through thin tubes (called ureters) into your child's bladder.

How female-to-male gender reassignment surgery works

The Epley maneuver or repositioning maneuver is a maneuver used to treat benign paroxysmal positional vertigo of the posterior or anterior canals

MRCPCH Clinical Revision - more videos at http://mrcpch.paediatrics.co.uk
Revise for your MRCPCH Clinical exam, with videos and high quality content created by the London Paediatrics Trainees Committee.
Examiner: Jonathan Round
Candidate: Amitav Parida
Filming: Mary Chesshyre, Huey Miin Lee, Chris Kelly
Thank you to the Evelina Children's Hospital for allowing us to film during their MRCPCH Revision Course (https://www.guysandstthomaseve....nts.co.uk/mrcpch-cli

Male and female Foley catheter insertion into bladder. Using mannequins.

A video describing the procedure of colonoscopy or flexible fibre-optic examination of the colon.

#ComprehensiveClinicalClass
History, Examination and Management of Hernia
Mentor: Dr. Nishanth, Consultant Surgeon, Bengaluru.
THE WHITE ARMY
To make studies more interesting and enjoyable, we are constantly trying to share most important tables, charts, diagrams, mnemonics, scoring systems, diagnostic criterias, motivating quotes and other useful study materials on
ANDROID APP - All in 1 Free Medical Education App for Medicos
https://play.google.com/store/....apps/details?id=com.
INSTAGRAM PAGE
@the_whitearmy
https://www.instagram.com/the_whitearmy/
TELEGRAM GROUP
PDFs, PPTs and other study materials stored for easy, convenient access and download.
https://t.me/whitearmyofmedicos
Anyone interested to present clinical cases, willing to join whatsapp discussion group, can send a mail to whitearmyofmedicos@gmail.com
#StudyManiaInSocialMedia
#HelpOthersToHelpOurselves
#StudyEnjoyingEnjoyStudying
DISCLAIMER
THE WHITE ARMY does not own or claim to own any of the media used in the following video/stream. The media belong to their respective owners who may have copyright over them.The media have been taken from various sources and are used for medical educational purposes only. The following video/stream may contain images that may not be suitable for all audiences, viewer discretion is advised.
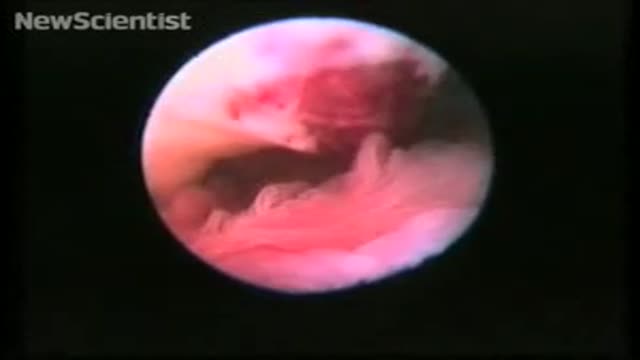
To record the sequence, Stephan Gordts and Ivo Brosens of the Leuven Institute for Fertility & Embryology in Belgium performed transvaginal laparoscopy, which involves making a small cut in the vaginal wall and observing the ovary with an endoscope.
"This allows us direct access to and observation of the tubo-ovarian structures without manipulation using forceps," says Gordts.
For the photos of ovulation, which only accidentally captured the critical moment, Jacques Donnez at the Catholic University of Louvain (UCL) in Brussels, Belgium, used gas to distend the organs for photography. However, Gordts and Brosens planned the procedure to coincide with ovulation and used saline solution to "float" the structures.
Perfect timing
Observation was timed for the day of the peak of the patient's luteal hormone cycle. Ovulation was predicted to occur on the evening of the day of the LH peak, and the endoscope introduced at 6 pm.
A small amount of saline was used to float the opening of the fallopian tube, its fimbriae (the "fingers" that sweep the egg into the tube) and the ovary itself. This gives a more natural appearance than gas, says Gordts.
In the video, the fimbriae can be seen sweeping in time with the patient's heartbeat. A mucus plug can be seen protruding from the ovary – this contains the egg.
"The ovum is not captured 'naked'," says Gordts. "There is no eruption like a volcano."
Gordts says that in clinical practice it is not easy to organise the observation of ovulation. "We were probably lucky to be successful at our first attempt," he says.
Draining Huge Back Cyst

Dr. Alex Campbell and Dr. Carolina Restrepo of Premium Care Plastic Surgery in Cartagena, Colombia perform a Mommy Makeover on an international patient. Watch the procedure as Dr. Campbell and Dr. Restrepo work together to offer this patient more surgery in less time, which leads to a quicker recovery and better results.
