- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Open Appendectomy Surgery Video

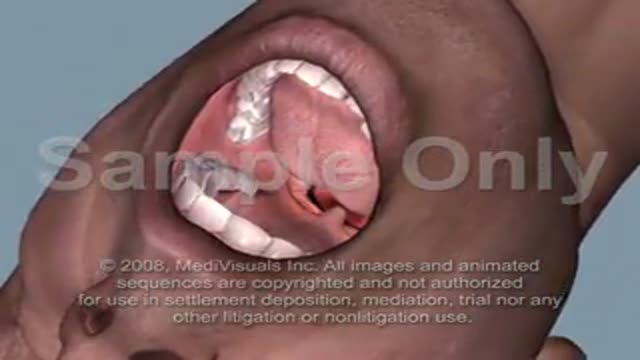
Foreign Body(FB) Airway (Whistle) was inhailed by a child causing intermitent stridor & respiratory distress.FForeign Body was removed successfully by rigid endoscopy under General Anesthesia (G/A).The relevant steps of procedure are shown
Endotracheal Intubation Sample Animation

Hematoma Removal! Surgery, Blood, Popping
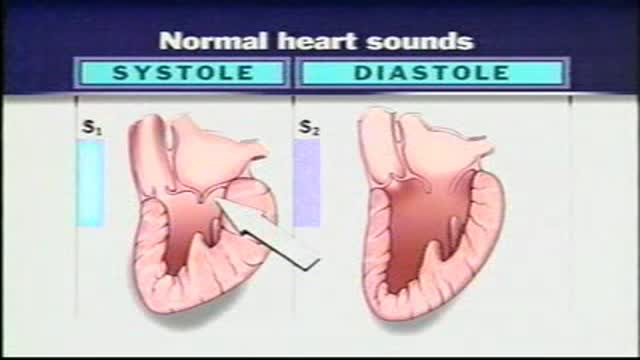
Normal Heart Sounds With the aid of a stethoscope you can hear the characteristic sounds of the normal heartbeat, typically described as a "lub-dub." These sounds are produced by the closure of the heart valves. The first heart sound or "lub" results from closure of the tricuspid and mitral valves. It is a rather low-pitched and a relatively long sound which, as indicated in, represents the beginning of ventricular systole. The second heart sound, or "dub," marks the beginning of ventricular diastole. It is produced by closure of the aortic and pulmonary (pulmonic) semilunar vanes when the intraventricular pressure begins to fall. This "dub" sound is typically heard as a sharp snap because the semilunar valves tend to close much more rapidly than the AV valves. Because diastole occupies more time than systole, a brief pause occurs after the second heart sound when the heart is beating at a normal rate. Therefore, the pattern that one hears is one of: "lub-dub" pause, "lub-dub" pause, and so on. Sometimes, especially in young normal individuals, a third heart sound can be heard. This sound is produced by the very rapid influx of blood into the partially filled ventricle. It is typically very faint and as such difficult to hear.

-The cremasteric reflex test is considered positive if there is elevation of the testis in response to stroking the upper inner thigh. This reaction is typically absent in testicular torsion and boys under the age of 6 months. Although not completely reliable in older boys and adults, an absent cremasteric reflex is highly suggestive of torsion. Patients with epididymitis usually have a normal cremasteric reflex, with pain and swelling isolated to

Watch that video to know How to Remove Blackheads From Your Nose

This video shows how to insert a chest tube

"The act of cutting off the prepuce or foreskin of males, or the internal labia of females." Webster's Revised Unabridged Dictionary (1913)

This is the incredible moment a new-born baby arrived still inside its amniotic sac, completely intact. The tiny infant can be seen moving and stretching still inside the sac, as medics prepare to snip the new born free. The amniotic sac is a thin but durable membrane filled with fluid which helps keep a baby warm and safe from bumps during pregnancy. When it breaks, this is typically referred to as a woman's 'waters breaking' shortly before she gives birth. But in rare cases, less than 1-in-80,000 births, the baby is delivered with the membranes still intact and this is known as a 'caul birth'. Some babies are born with part of the membrane still attached to them, but to be born completely encased in the intact membrane is incredibly rare. Many people still believe the phenomenon to be a good omen for the child's infancy and it is has even been suggested, but not proven, that caul babies will always have a natural affinity for water. The video was taken in Spain on Saturday and captures the rare moment the baby was born with the membrane covering its entire body, just minutes after its twin was delivered normally.

watch that video of Navel stone removal from a dirty bellybutton

Midline Episiotomy

Breast augmentation is a surgical procedure to enhance the size and shape of a woman's breasts for a number of reasons: To enhance the body contour of a woman who, for personal reasons, feels her breast size is too small To restore breast volume lost due to weight loss or following pregnancy To achieve better symmetry when breasts are moderately disproportionate in size and shape To improve the shape of breasts that are sagging or have lost firmness, often used with a breast lift procedure. By inserting an implant behind each breast, surgeons are able to increase a woman's bustline by one or more bra cup sizes.

Always consult your doctor and seek help early enough to prevent complications

A very bad lasik eye surgery duringwhich the surgeon messed everything

Occiput or cephalic — the baby's head is down, and the baby is facing the mother's abdomen. This position results in back pain and a prolonged labor. Transverse — the baby is lying crosswise in the uterus, side-to-side over the mother's pelvis, in a horizontal position rather than vertical.

The thyroid is a butterfly shaped gland overlying the voice box and the windpipe. Adjacent to the thyroid are the parathyroid glands which control the body's calcium and the recurrent laryngeal nerves that control the voice box muscles. The thyroid is removed while preserving the recurrent laryngeal nerves and the parathyroids.
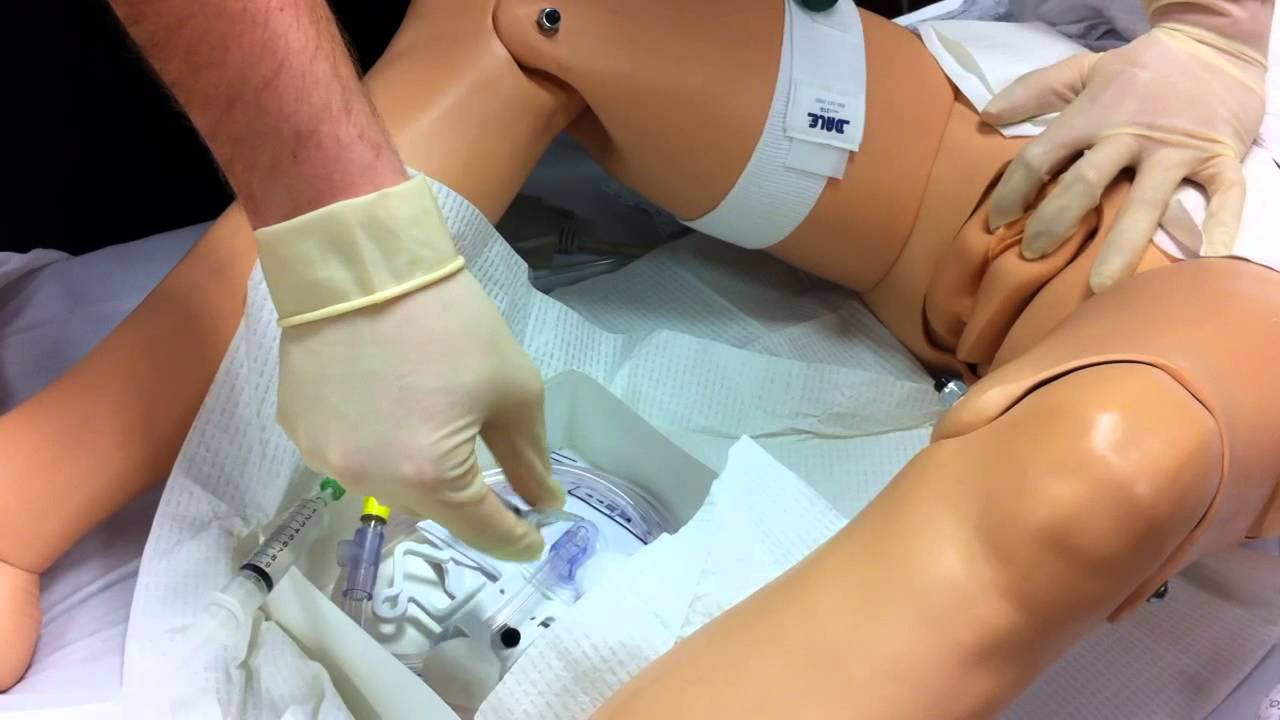
Watch that Female Foley Genital Catheter Insertion Procedure
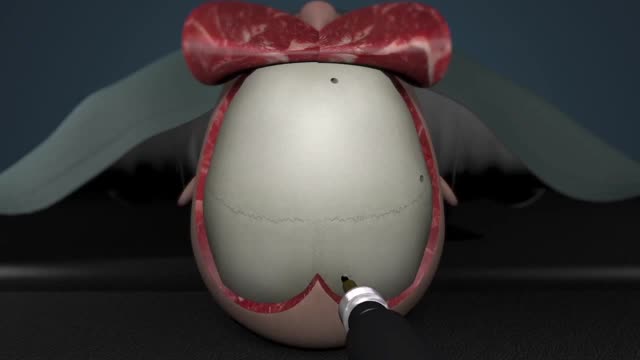
A craniotomy is the surgical removal of part of the bone from the skull to expose the brain. Specialized tools are used to remove the section of bone called the bone flap. The bone flap is temporarily removed, then replaced after the brain surgery has been done.

A video showing how to do Spinal Anaesthesia
